Consent Form Pm 330 Spanish

Pm 284 Form Fill Online Printable Fillable Blank Pdffiller
Http Files Medi Cal Ca Gov Pubsdoco Forms Pm 330 Eng Sp Pdf
Sterilization Consent Form California Non Federally Funded Fill

Sterilization Form Fill Online Printable Fillable Blank

Sterilization Consent Form California Non Federally Funded Fill
Https Files Medi Cal Ca Gov Pubsdoco Outreach Education Workbooks Hap 2018 Pdf
State of california health and human services agency consent form pm 330 department of health services nota.
Consent form pm 330 spanish. Providers must supply their npi number when ordering the form s. Sterilization consent form pm 284 authority. Your sterilization consent form pm330 my doctor online the. The form begins with a cover page describing the purpose of the form and its expiration date.
Mc 4035 04 08 sp medi cal consent form. Consent form pm 211. Sillen bilateral tubal ligation bilateral tubal ligation bilateral tubal ligation bilateral tubal ligation marcus j. Consent for sterilization created date.
Sterilization consent pm 330 forms in english and spanish can be downloaded from the forms web page of the medi cal website or can be ordered by calling the telephone service center at 1 800 541 5555. The only acceptable sterilization consent form is the department of health care services consent form pm330. Samples english and spanish may be found at the link at the end of this bulletin along with instructions for completing the form. Pm 284 form state of californiahealt h and human services agency california department of public health sterilization consent form nonfederally funded notice.
Ninguno de los beneficios que recibo de los programas o proyectos subsidiados con fondos federales se me cancelará o suspenderá en caso de que yo decida no esterilizarme. Before obtaining consent the person who obtains consent must provide the individual to be sterilized. Example of pm 330 sterilization consent form penny l. Male sterilization booklet from dhcs spanish female sterilization booklet from dhcs english female sterilization booklet from dhcs spanish instructions for sterilization consent form pm 330 sterilization consent form pm 330 list of reportable diseases department of public health claims settlement practices provider packet fair.
Title 22 california code of regulations ccr sections 70707 1 70707 7 this afl is being issued to remind facilities where they may obtain the sterilization consent form which is specifically required for use by hospitals but is also available to all health facilities and clinics. Department of health services. Fields 21 22 cross off the paragraph which does not apply fields 27 28 physician signature date must be. Statements are also included for an interpreter a person obtaining consent and a physician.
Mydoctor consent form. Spanish pre enrollment application dhcs 4073 tagalog pre enrollment application dhcs 4073 vietnamese provider data sheet pm 177. Mc information notice 002 09 07 sp summary medi cal eligibility 2 18mb mc information notice 003 11 12 sp early and periodic screening diagnosis and treatment services.
Https Www Hhs Gov Opa Sites Default Files Consent For Sterilization English Updated Pdf
Http Jre Sagepub Com Content 11 1 31 Full Pdf

Pm 284 Form Fill Online Printable Fillable Blank Pdffiller
Pdf Gender Stereotypes In Spanish Television Commercials
Https Www Molinahealthcare Com Providers Ca Pdf Medical Medi Cal Provider Manual 2019 Pdf

Pdf Adaptation Of Child S Report Of Parent Behavior Inventory
Pdf Exercise Is The Real Polypill
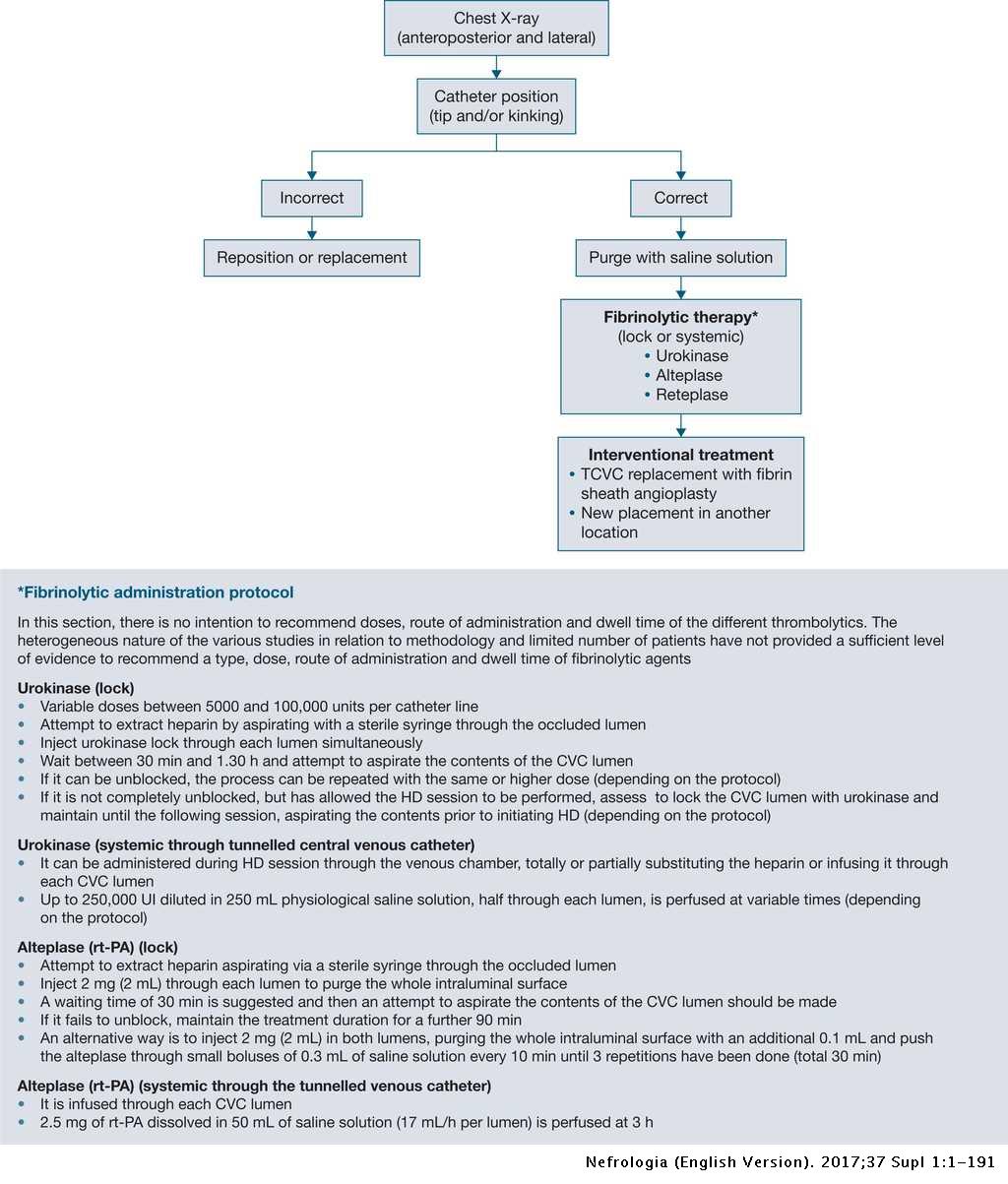
Spanish Clinical Guidelines On Vascular Access For Haemodialysis
Https Www Iehp Org Media Documents Providers Provider Resources Manuals Medicare 2020 07 Medical Records Requirements Ashx La En Hash 9aa23006c3db231d549f141a19ed98c146e7a9c5
Psychopharmacologic Behavioral And Psychotherapeutic Approaches

Wo2019229658a1 Entpd2 Antibodies Combination Therapies And
Https Files Medi Cal Ca Gov Pubsdoco Outreach Education Workbooks Hap 2020 Pdf
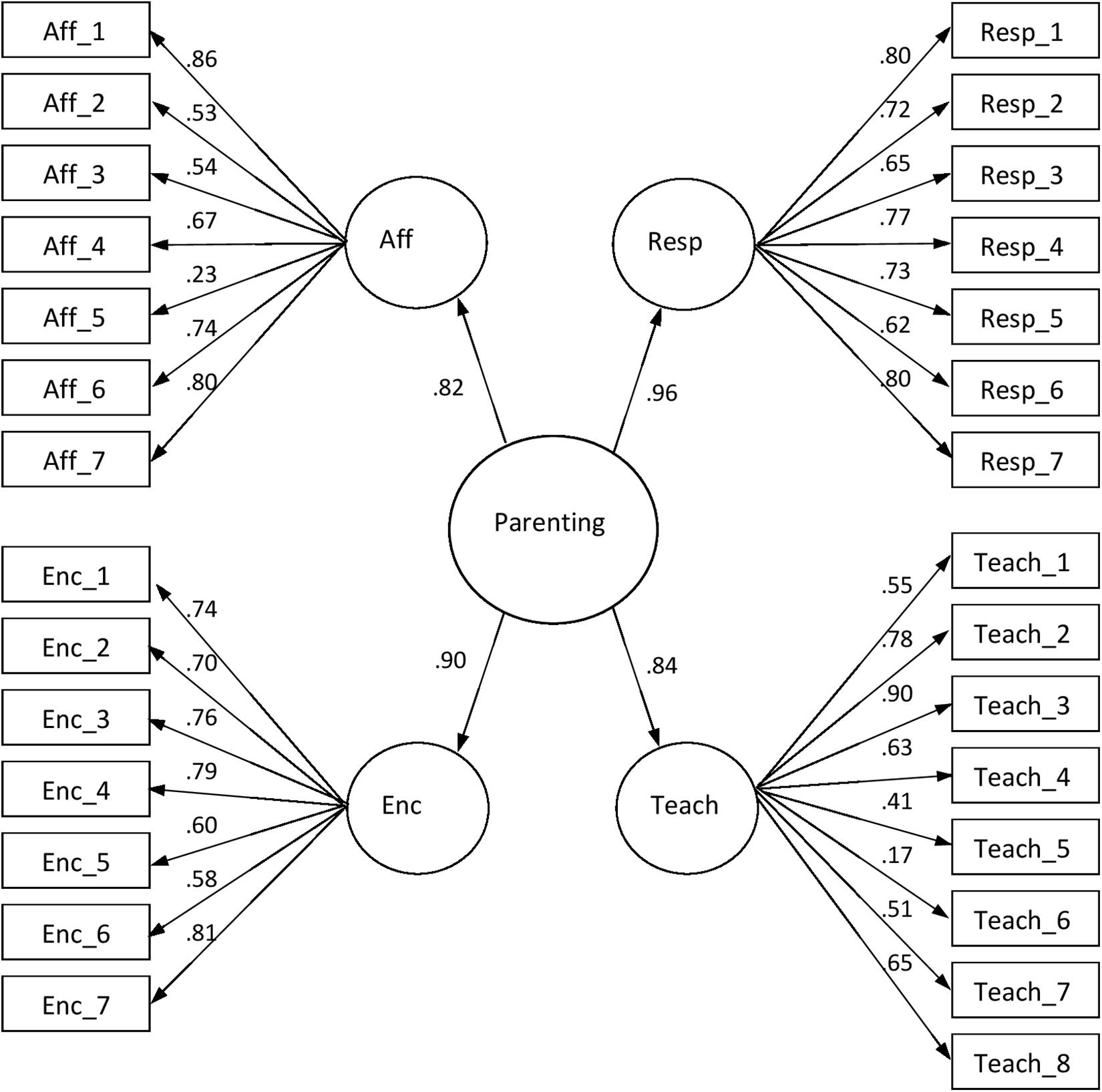
Frontiers Spanish Validation Of The Piccolo Parenting